
How will AI transform the field of genetic counseling?
Thinking...
Instead of the usual question, “Will AI replace genetic counselors?” we should be asking:
Which parts of genetic counseling will AI augment, and what will that free genetic counselors up to do?
By augment, I mean AI handles the repetitive steps, while humans remain responsible for interpretation, decisions, and support. AI is a tool to streamline parts of the work, so human expertise can go deeper and reach more people overall.
Patient intake
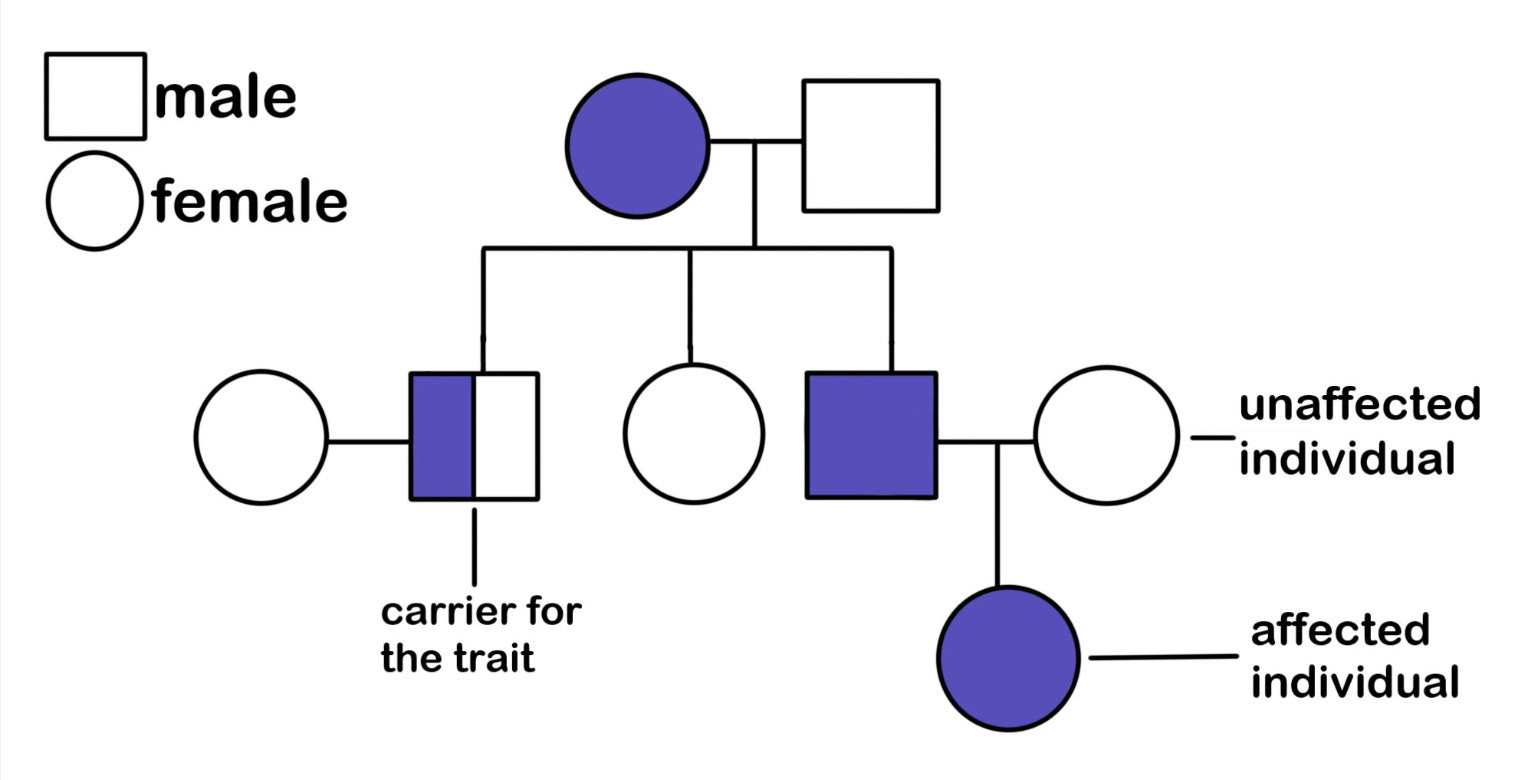
We can all admit that the practice of taking a family history by manually drawing a pedigree (example above) is a bit archaic and time-consuming.
It is easy to imagine a near future where patients share their family history with (HIPAA-compliant) AI ahead of the appointment, whether through a chatbot, an avatar, or another tool. The technology could organize the information, build a draft pedigree, and flag potential patterns the way we do.
A reasonable concern that I’ve heard from colleagues is:
“But the pedigree is how I build rapport with patients. We can’t replace basic human connection with technology.”
This concern is, of course, valid. We’ve held onto the practice of creating a pedigree for a reason. Reviewing our patient’s family history, person by person, allows us to quickly learn about:
Relationship dynamics
Life experiences
Communication styles
Still, having AI draft the intake does not mean the human part disappears. It simply changes where it happens. We can return with thoughtful follow-up questions, clarify details that matter, and spend more time on personalized care and guidance. And, we can build trust in other ways too, some of which will be discovered once we are not anchored in pen-to-paper circles and squares.
Patient education
Many of us explain the same concepts multiple times a day, just tailored to different patients, goals, and levels of baseline knowledge.
Because of that, there are parts of counseling that can, and arguably should, become more automated over time.
The true “no-brainers” for AI
These are the questions that do not require deep clinical judgment or emotional support, and they take up real visit time:
Logistics: How long does testing take? How do I submit my sample? What happens next?
Billing: What does it cost? Will insurance cover it? What are the self-pay options?
The next layer AI could also handle well
When it comes to pre-test counseling and post-test counseling (for negative/normal results), AI could likely deliver a large portion of education-based content in a clear, consistent, and scalable way, especially when built with solid guardrails and human oversight:
What information can we learn from this genetic test?
What are the benefits and limitations of testing?
What do negative/ normal results mean?
What does a variant of uncertain significance mean in general terms?
What does “residual risk” mean after screening?
Education is not the same as counseling
I’m pointing out a distinction that matters: education is explaining information. Counseling is helping someone use that information to make decisions, process emotions, and move forward in a way that aligns with their values and circumstances.
If AI could reliably take on the education and logistics, clinical genetic counselors could spend far more time with the patients who truly need support, maximizing their value. Fewer visits would be devoted to explaining the basics, and more time could go to the hardest conversations, the most complex cases, and the people processing difficult news in real time.
Where the human genetic counselor remains essential (in my 2025 opinion…)
I believe patients benefit most from a real genetic counselor when results or circumstances are high stakes or uncertain, including:
High-risk, unexpected, or abnormal results
Rare or clinically nuanced cases
Gray-area / uncertain results
Situations with complicated family dynamics, trauma, prior loss…
Genetic counselors add unique value in helping patients navigate decision-making, with questions like:
Should I have an amnio?
Should I get tested given my specific hesitations and concerns?
Should I share my results with family members who are also at risk?
And there are parts of this work where I personally do not think human-to-human connection is replaceable:
Helping patients process complicated emotions
Supporting families through conflict or guilt
Being truly present with another person in a high-stakes moment
I do realize, though, that AI will continue to get better at handling nuance, supporting values-based decision-making, and even straight-up counseling. Some people already advocate for the use of full AI therapy models. It’s inevitable that people will disagree on where the line should be, which is why this work must be guided by ethical thinking and extensive research.
Variant interpretation
Variant interpretation is deciding whether a DNA change is meaningful (linked to disease) or just normal human variation.
And I’ll say it: variant interpretation is both an art and a science. Two qualified clinicians can look at the same variant and weigh the evidence differently, especially when the data is limited or mixed.
Even today, AI-assisted tools are used to:
Pull together evidence from many sources in one place
Quickly scan research papers to surface similar cases
Estimate whether a DNA change might matter (for example, whether it could disrupt how a gene works)
That said, we are not ready to fully rely on AI to make final variant classification calls today. Meaning, we cannot fully trust AI to call a specific genetic change “disease-causing” or “benign.”
Over time, AI will likely get much better at connecting phenotype to genotype, summarizing evidence, and finding the most relevant literature in seconds. I do not think it will replace variant scientists. I do think it will become the default first pass, giving scientists a strong starting point and leaving humans to make the final call.
Literature review / finding similar cases
Right now, when we encounter a rare variant and need to find comparable cases, we typically turn to:
PubMed
Google Scholar
Public and private databases
Internal institutional knowledge and lab contacts
AI has the potential to compress this workflow dramatically by quickly surfacing the most relevant papers and case reports, especially those that match the same variant, gene, phenotype, or key clinical details.
One important caution: AI can and does fabricate citations and even entire papers. Any AI-assisted literature search still requires a human to verify the sources, read the originals, and confirm that the evidence is real and accurately represented.
Phenotyping
Phenotyping is the process of carefully describing a person’s observable traits and medical features (symptoms, exam findings, imaging results, lab values, and physical characteristics). It helps us recognize patterns and link them to possible genetic conditions.
AI can help by:
Comparing a patient’s set of features to thousands of known patterns
Spotting subtle physical clues that could (potentially) be missed in clinic
This point needs still to be proven, but it’s theoretically possible.
There are already tools including Face2Gene, which uses AI to analyze a patient’s facial features (along with key clinical findings) and suggests a shortlist of genetic syndromes to consider.
Importantly, AI will be used as decision support, not a diagnosis, and any “match” still needs clinical judgment and confirmatory genetic testing.
Identifying referrals
If we’re honest, one of the biggest issues in the field is getting the right patients to genetics in the first place.
In a future electronic medical records system, I can easily imagine software that flags:
Symptom clusters that are more likely to have a genetic cause
Family history patterns suggestive of hereditary disease
Prenatal findings that meet criteria for specific testing, referrals, or follow-up
This kind of system could standardize genetics referrals by reducing reliance on any single provider to remember every indication, while still leaving the final decision to the clinician.
Documentation
I have yet to meet a healthcare provider who enjoys writing notes.
HIPAA-compliant note drafting systems are already emerging, and the impact is obvious:
Cleaner notes
Less time charting
More time with patients
The best version of this future is not AI writing the final record on its own. It is a workflow where AI drafts and genetic counselors edit, keeping the note accurate, nuanced, and clinically responsible.
What could go wrong?
Before we get carried away, it’s worth naming the risks if we automate carelessly:
Fake citations
Major bias (who gets flagged for referral)
Over-reliance and deskilling
Privacy / data ownership issues
Patients misunderstanding chatbots as medical advice
…And certainly more
These risks are reason to build carefully, test rigorously, and design for safety from the start.
Where might this leave us?
The way I see it, the future is not “less genetic counseling.” It will be a wider reach, with genomics embedded across more areas of medicine.
If AI can take on the repeatable work, it creates space for genetic counselors to spend more time on what we do best:
Systems-level genomics implementation and service design
Equity-focused access work and advocacy
Research, publications, and guideline development
Teaching other medical specialties how to use genetics responsibly
And of course, the most complex clinical cases
One note for anyone building in this space: it helps to involve genetic counselors early (if you’re not one already). GCs can offer real-world insight into patient needs, clinic workflows, and the places where language, education, and support matter most. And given the risks of automating healthcare too quickly, that perspective can be a useful safeguard.
Really thoughtful framework for thinking about AI augmentation versus replacement. The distinction between education and counseling is crucial becuase one can be standardized while the other requires human judgment in real time. The phenotyping and referral flagging use cases are especially promising since they address upstream access bottlenecks not just downstream efficency gains.